
Boys in South Sudan use ‘pipe filters’ to consume water without ingesting Guinea worm larvae.Credit: L. Gubb/The Carter Center
In 2006, a contested region of southern Sudan that had been embroiled in a long civil war recorded more than 20,000 cases of Guinea worm disease, 80% of the world’s total. Last year, the now independent nation of South Sudan reported just two cases of the parasitic infection, down from five the previous year.
The drastic decline has been achieved thanks to an eradication programme that relies, in large part, on community-based volunteers. When South Sudan became independent in 2011, there was little infrastructure and the new government’s institutions did not have the capacity to send trained staff to areas affected by the parasite, says Makoy Samuel Yibi, director of the Guinea worm eradication programme at the country’s Ministry of Health. “From the outset, the design of the programme was anchored on the structures of the community,” Yibi says.
Globally, Guinea worm has declined from an estimated 3.56 million cases across 20 countries in 1986 to just 14 human cases in 5 countries in 2023 — mostly through bottom-up, low-technology efforts similar to those in South Sudan. What’s more, this has been achieved despite the lack of a vaccine or drug treatment for the parasite. The Guinea worm eradication effort shows the power of relatively simple, non-pharmaceutical interventions that emphasize improved hygiene and community empowerment. But a series of unexpected setbacks over the past decade and a half have kept total eradication just out of reach, demonstrating the unpredictability of the disease.
Cycle of misery
Guinea worm disease, also known as dracunculiasis, is caused by the roundworm Dracunculus medinensis (see ‘The Guinea worm life cycle’). People in remote communities in Africa who lack access to safe water supplies can unwittingly ingest water containing tiny crustaceans called copepods that harbour the worm’s larvae. These larvae then burrow through the wall of the human digestive tract and mature in the abdominal cavity, where male and female worms find each other and mate.
Most people who are infected are unaware of it until, after about a year, the pregnant female worm migrates to the surface of the skin and begins to emerge through a painful sore, usually on the legs or feet. When people immerse the sore in water — either seeking relief for the itching, burning wound or simply during daily chores such as collecting water or washing clothes — the worm releases millions of larvae into the water and the cycle begins again.
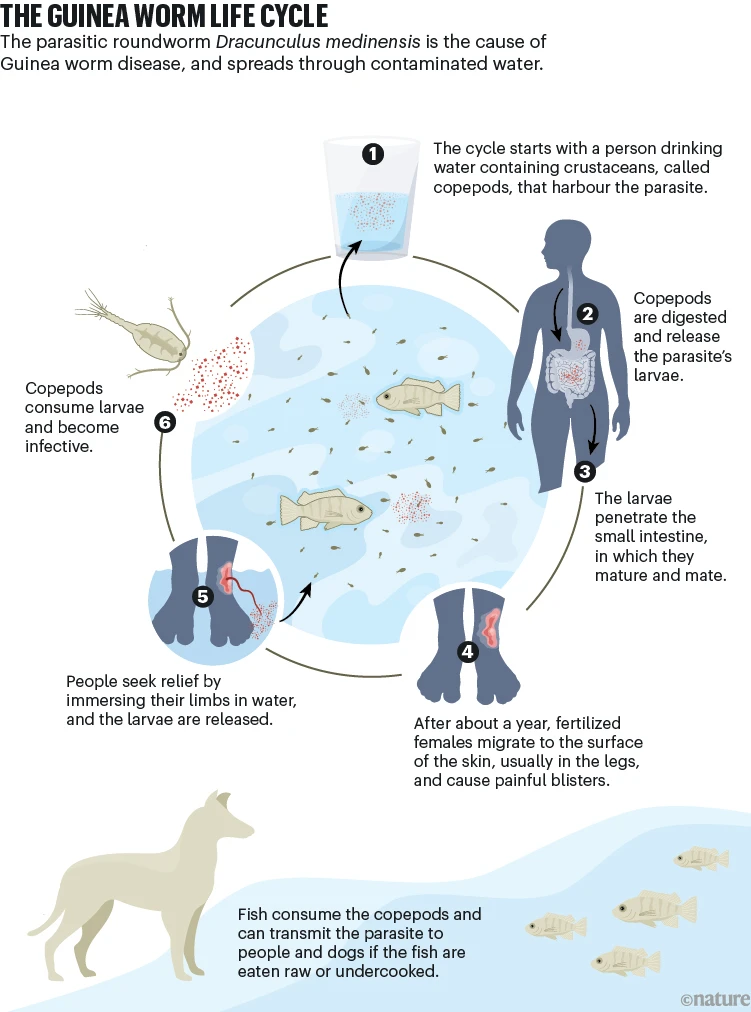
Infographic by Alisdair Macdonald
The parasitic infection itself is rarely fatal, but can hamper people’s activities for weeks or months at a time. The gradual emergence of the female worm, which can be one metre long, causes debilitating pain, and secondary bacterial infections can develop at the site of emergence. Affected adults might be unable to plant or harvest crops and children might be unable to go to school, putting livelihoods and access to education at risk in already under-served areas. Infection does not confer immunity to the parasite, and in the past many people in affected communities contracted Guinea worm year after year after year.
Guinea worm has been around for millennia. The disease is mentioned in Egyptian medical texts dating to 1,550 bc, which also describe the treatment that is still standard today: winding the emerging worm around a small stick and painstakingly pulling it out centimetre by centimetre over the course of weeks. This is a delicate task that can’t be rushed, because if the worm breaks and remains partly inside the body, serious secondary infections can ensue.
Previously, Guinea worm was widespread across South and Southwest Asia and Africa. An estimated 48 million cases occurred annually worldwide in the 1940s; advances in sanitation brought the numbers down over the next several decades to just a few million per year. Then, in 1986, the Carter Center, the humanitarian non-profit organization launched by former US president Jimmy Carter, took over and expanded a global eradication programme that had been started six years earlier by the US Centers for Disease Control and Prevention (CDC). Guinea worm was the first parasitic disease targeted for eradication and the only disease for which an eradication programme was launched in the absence of a drug or vaccine.
Community-led campaigns
As well as the Carter Center and the CDC, the Guinea worm eradication programme involves international bodies such as the World Health Organization and the United Nations children’s charity UNICEF; national ministries of health in those countries where Guinea worm is present; and outside humanitarian volunteers. But at the programme’s core are the village volunteers who identify and help to care for people with Guinea worm disease, and who provide education and resources to enable the community to interrupt the parasite’s life cycle.
The approach is very different from the military-style, top-down strategy that characterizes many disease-eradication campaigns, says Jonathan David Roberts at the University of Leeds, UK, who is studying the history of disease-eradication efforts. The drives to eliminate Guinea worm, he says, have been powered “largely by ordinary people doing relatively small things within their own communities”. And that, he says, is a big part of their power: “The participatory approach of people solving their own problems can actually be a really effective health intervention.”
Village volunteers go out into the community every day to look for Guinea worm cases. Infections are reported up the chain to the national health ministry, and pain medication and wound care are provided to help to minimize the risk of secondary infection. A key task is to prevent people with Guinea worm from entering ponds and other water sources and thereby contaminating them with larvae.
The other piece of the puzzle is helping community members to avoid consuming water that might contain Guinea worm larvae. One solution is to give households in affected communities a fine mesh fabric that can be used to strain copepods from the water supply. But for people such as herders, refugees or those in a nomadic community, such filters can be impractical. Instead, they’re given pipe filters — essentially straws with a fine mesh across one end that can be used to drink safely from a water source.

A Ghanaian volunteer demonstrates how to filter water.Credit: Emily Staub/The Carter Center/CDC
With their deep, embedded understanding of the local community, village volunteers “use the local sentiment and religious and cultural context as part of their story, as they encourage the adoption of behaviour change”, says Adam Weiss, director of the Guinea worm programme at the Carter Center.
In a paper published last year1, Roberts catalogued many of the ways in which countries and communities have adapted the global Guinea worm eradication programme to suit local conditions. In Ghana, for example, workers developed simple, picture-based documents so that people who can’t read can serve as volunteers, leading to an increase in the recruitment of women. In Burkina Faso, communities established a new village authority known as bouilla naba or ‘chief of the pond’, charged with maintaining and guarding village water sources. Often, this responsibility is given to older men as a way for them to continue to contribute to community well-being despite perhaps being unable to undertake heavy physical labour, Roberts says.
Building local capacity in these ways has benefited health-care infrastructure more broadly in many sub-Saharan African nations, Weiss says. The legacy of anti-Guinea worm efforts can be seen in “community-based surveillance systems that cover multiple diseases”, he says. “They might track maternal and infant deaths, they track malaria — they can do all types of different things.”
South Sudan’s Guinea worm programme involved more than 20,000 community-based health workers at its peak, Yibi says. Many of these individuals later underwent further medical training and still work in health care, providing a variety of services. In 2016, the country’s Ministry of Health adopted a community-based health system modelled on the Guinea worm programme. “In many of the locations where we are effectively interrupting transmission, the team has now been completely integrated and assimilated into the health sector,” Yibi says.
Eluding eradication
So far, the WHO has certified 200 countries around the world as free of Guinea worm. Since 2015, fewer than 60 cases have been reported annually worldwide, and there have been fewer than 30 annually since 2020.
The parasite is still classed as endemic in five countries in a belt across equatorial Africa: Angola, Chad, Ethiopia, Mali and South Sudan. And recent years have also seen the emergence of new challenges that have kept global eradication of the parasite frustratingly out of reach. In 2010, Guinea worm infections were rediscovered in Chad, after a decade without any cases, and these infections were soon traced to domestic dogs.
Since then, Guinea worm infections have been found in domestic dogs and cats in parts of Chad, Mali and Ethiopia, as well as in olive baboons (Papio anubis) in Ethiopia. There have been sporadic reports of Guinea worm in other species in the past, but scientists assumed these were just occasional spillover events from human hosts. New reports indicate, however, that the worm is now much more widespread among animals — and researchers think that this represents a shift in the parasite’s ecology. Maryann Delea, senior associate director of research for the Guinea worm programme at the Carter Center, thinks that her team would have come across animal infections earlier if they had been occurring at currently detected levels. “We have pretty strong surveillance systems out in endemic areas. We have people out going house to house every day in affected communities,” she says. “We would have picked it up.”
Land-use change, climate change, changes in human or animal behaviour, or even an expansion in the types of intermediate hosts that can be infected with guinea worm could all be driving this move towards animal infections. It might be impossible to find out for certain, Delea says.
Regardless of how it came about, evidence now suggests an extra transmission pathway for the parasite2. Aquatic animals such as fish and frogs can harbour high numbers of the copepods with Guinea worm larvae in their guts, or possibly even the worm in their tissues. Dogs (and people) can then become infected when they eat the uncooked (or undercooked) animals.

A parasite is examined under the microscope to verify the presence of Guinea worm.Credit: Jane Hahn/The Carter Center
The emergence of Guinea worm infections in non-human animals has posed a huge challenge to the eradication programme. One reason the parasite had been seen as a good candidate for eradication in the first place was that it was thought to affect humans almost exclusively. Diseases are always harder to stamp out if they can circulate in multiple species.
In areas where domestic-animal infections are prevalent, they are now driving the persistence of Guinea worm in humans, studies suggest3. Reports of animal infections increased from 685 in 2022 to 878 in 2023, which the Carter Center attributes to increased surveillance in Angola and Cameroon. Meanwhile, infections among dogs in Chad fell for the fourth year in a row. In 2019, the WHO’s target date for Guinea worm eradication was pushed back from 2020 to 2030, in part in recognition of the challenge posed by animal infections.
But according to Weiss, the goal of the programme hasn’t changed: “The endgame remains getting to zero in all hosts, unless the science tells us otherwise,” he says.
Animal opportunities
If animal hosts are driving continued circulation of Guinea worm, then wiping out the parasite — altogether, or even just in humans — requires addressing infections in animals. Many of the low-tech, non-pharmaceutical strategies that drove down human guinea worm infections to near zero are now being adapted and applied to controlling these animal infections. For example, community volunteers have begun to monitor dogs for signs of Guinea worm infection. And people in areas where animal infections are prevalent are being encouraged to tether domestic dogs (and sometimes cats) to prevent them from either drinking contaminated water or entering water sources if they show signs of infection.
People are also being encouraged to refrain from feeding dogs the entrails of fish they catch — which had been a common practice in some areas — and to dispose of aquatic-animal waste in secure pits so that any Guinea worm larvae they might harbour cannot enter water sources.
At the same time, there has been increased use of temephos, a larvicide, to reduce the number of copepods in shallow standing water. After all, “you’re not going to get a dog to drink through a straw”, says Claire Standley, a global public-health researcher at Georgetown University in Washington DC.
Standley is not directly involved in Guinea worm eradication, but has worked on other neglected tropical diseases (NTDs) with animal hosts, such as schistosomiasis. She says that Guinea worm efforts have contributed significantly to the emergence of a ‘One Health’ approach4 — one that seeks to leverage the connections between human, animal and environmental health — across NTDs generally.
The emergence of Guinea worm infections in animals has, over the past decade, kicked off a surge in basic research into the parasite’s biology and ecology, which researchers aim to translate into diagnostic tests and perhaps, eventually, pharmaceutical treatments. Had infections in animals not surged, the existing toolkit of behavioural interventions aimed at humans could well have eradicated the parasite, Delea says. But the landscape has changed.
Several trials have investigated flubendazole, a deworming medication, for preventing Guinea worm disease in dogs. Results so far have been mixed5, but researchers are continuing to search for formulations and delivery methods that could yield a more reliable extended-release treatment to protect dogs.
Researchers also want to better understand the range of species that can serve as hosts of Guinea worm larvae, and the species that can be infected with the adult worms. They also want to understand more about the immune response to the parasite — in dogs as well as in humans — and what goes on inside the body before the worm emerges.
This information could contribute to the development of diagnostic tests to identify infections before the worm emerges. In turn, diagnostics would give early clues as to where cases of Guinea worm disease are likely to emerge, enable tethering of dogs to be carried out in a more targeted way, and guide the use of an eventual therapeutic.

Children in Ghana study a book on Guinea worm disease.Credit: L. Gubb/The Carter Center
Detecting the presence of Guinea worm in the environment would be a significant advance. This, too, could give clues about where cases are likely to emerge and help to tailor preventive interventions. It would also aid efforts to certify countries as Guinea worm-free, which is more complicated in an era of animal infections.
The WHO published preliminary standards for both types of test late last year, but it will be challenging to develop approaches that are accurate, are practical in real-world conditions and offer a fast turnaround. The roll-out is likely to be an iterative process, says Delea, with tests that meet minimal standards moved into use as quickly as possible and then refined over time. A test to detect an immune response to a Guinea worm antigen, known as DUF148, has shown promise in laboratory studies6, but the method remains complex. Still, it’s a first step. “We’re really hoping that we will get something to the field by early next year,” Delea says.